- This topic has 0 replies, 1 voice, and was last updated 3 years, 3 months ago by
Anonymous.
-
AuthorPosts
-
April 6, 2021 at 5:55 pm #10215
Anonymous
InactiveAlright everyone, here’s the April ECG Case of the Month. New website and format so hopefully it translates well on here. Let me know if there are any issues/questions/comments
<span style=”text-decoration: underline;”>April 2021 ECG Case of the Month</span>
<span style=”text-decoration: underline;”>Case:</span>
Your patient is a 40 yo F who presents with fever, flank pain, 4 days of vomiting and inability to tolerate PO. She is dry appearing and tachycardic<span style=”text-decoration: underline;”>ECG:</span>
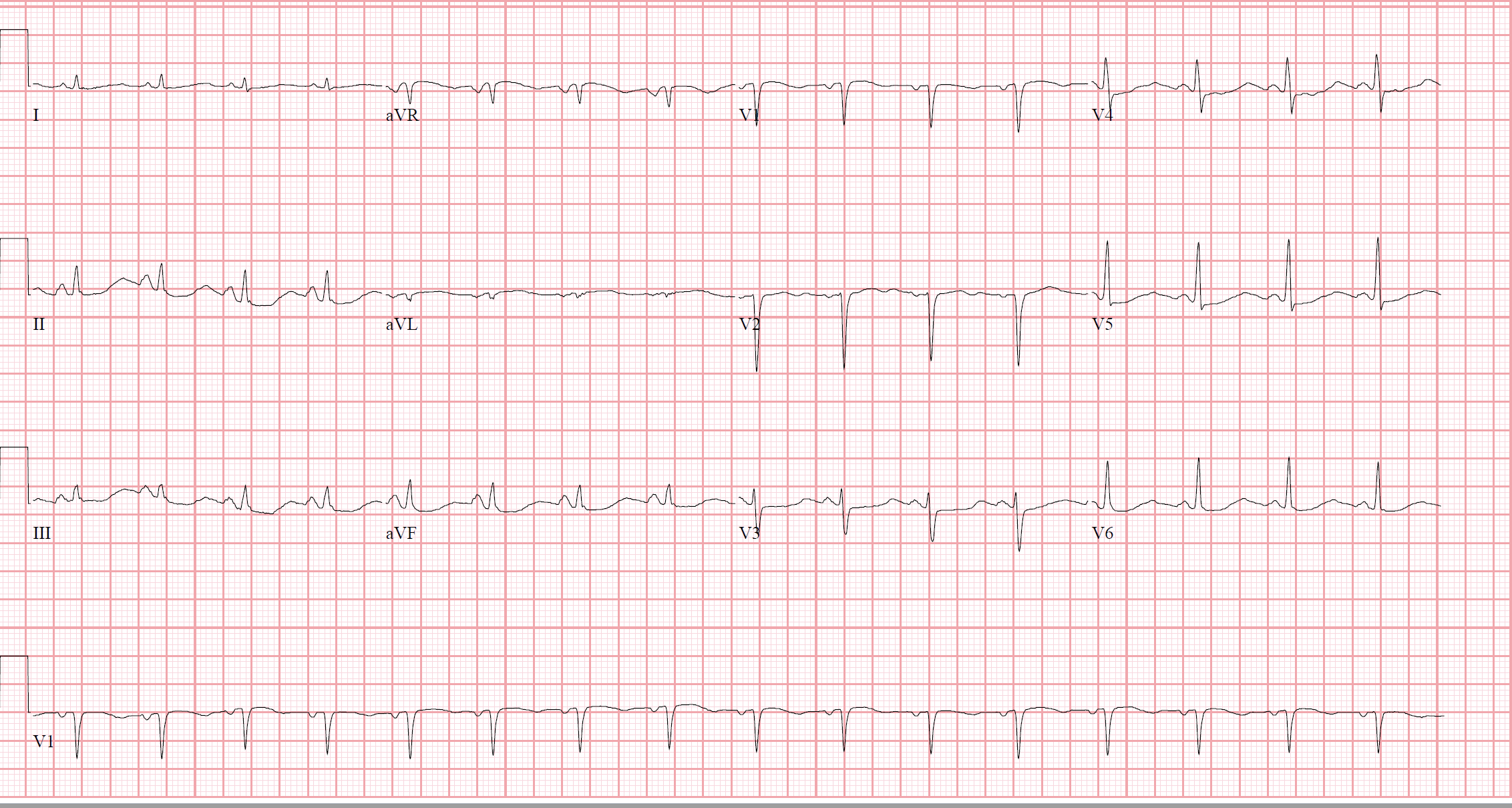
Interpretation:
Sinus rhythm, rate of ~100, axis is normal, PR interval is normal (~120msec), QRS is narrow, QTc appears long (calculated on ECG 577msec) with U waves V2. ST depression is present inferiorly, V3-6. QS waves V1-2.<span style=”text-decoration: underline;”>Cath/ECHO Results:</span> N/A
<span style=”text-decoration: underline;”>Clinical Course:</span>
The patient’s labs were remarkable for a urinary tract infection and potassium of 2.2 mEq/L (Mg 2.5 mEq/L). The patient’s clinical history and presentation and ECG findings are all accounted for by acute pyelonephritis complicated by hypokalemia and dehydration. The patient was resuscitated and she was admitted for observation, continued electrolyte repletion and telemetry monitoring<span style=”text-decoration: underline;”>Deep Dive:</span>
There are only a limited causes of ST depression:– Ischemia
– Digoxin use
– Hypokalemia
– Normal variant
– Result of preceding QRS complex (i.e., LVH with strain pattern)
– Rate related (commonly seen in SVT)Knowing the differential diagnosis of ST depression can be helpful. While ischemia is usually our first thought (and rightfully so), the only one on this list that applies to the clinical context of our patient is hypokalemia. This is further solidified with the other typical findings of hypokalemia on this ECG:
– Long QT (this is actually an inverted T-wave fusing with a more prominent U wave)
– Presence/increased amplitude of U waves (best seen in precordial leads)
– Flattened and sometimes inverted T-waves
– Peaked P waves in inferior leadsThere is no hard cutoff of potassium concentration that causes these ECG changes. However, if the potassium is <2.7mEq/L, they are more likely to have a collection of these findings1. All of these findings listed above should resolve once the potassium is repleted.
Of course, we are concerned about hypokalemia because it increases premature ventricular and atrial beats. This leads to supraventricular and ventricular arrhythmias, most concerning of which are VT/VF.
1 Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: 6th Edition.” Philadelphia, PA. Saunders/Elseviers. 2008
-
AuthorPosts
You must be logged in to reply to this topic. Login here